Clinical Workflow Signal Audit
A workflow intelligence demo for reducing ICU escalation delays caused by fragmented clinical signals.
ICU teams receive signals from vitals, labs, alarms, notes, handoffs, and clinician assessments. These signals often live across disconnected systems, causing delayed escalation and poor visibility during busy shifts. This project shows how fragmented ICU signals can become a structured audit trail, action-driven risk tiers, SLA routing logic, and a role-based dashboard.
- Domain
- Healthcare ops
- Focus
- Workflow intelligence
- Data
- Synthetic ICU
- Status
- Portfolio demo
ICU teams don't need more alerts. They need better signal flow.
More notifications add noise. The real gap is visibility into how signals move from generation to acknowledged action — and where that flow breaks down.
Fragmented clinical systems
Vitals, labs, alarms, and notes live in separate systems with no shared timeline.
Delayed escalation
Critical signals get noticed late because nothing tracks signal-to-action latency.
Documentation lag
Backdated notes and missing values hide the real timing of clinical events.
Handoff visibility gaps
Shift changes lose context about open risks, pending actions, and SLA clocks.
Data quality issues
Clock drift, impossible values, and partial entries silently degrade decisions.
Bed 12 — a 4-hour escalation window
A fictional ICU patient shows rising lactate, worsening tachycardia, and delayed documentation. The signals exist. They are just spread across labs, bedside monitors, EMR notes, and communication channels.
- +00:00GeneratedLactate trend rising in lab system
- +00:42DetectedBedside monitor flags tachycardia
- +01:55AcknowledgedNurse opens chart, no order placed
- +03:10Action initiatedResident notified via pager
- +04:05CompletedFluids ordered and started
A workflow intelligence layer, end to end
Each piece is intentionally focused on signal flow and operational accountability — not on making clinical diagnoses.
Synthetic ICU workflow dataset
Realistic, fully synthetic patient streams with no PHI.
Python data pipeline
Ingests, normalizes, and timestamps multi-source signals.
PostgreSQL schema
Audit-trail tables for signals, actions, and SLA events.
Data quality gate
Validates ranges, ordering, freshness, and completeness.
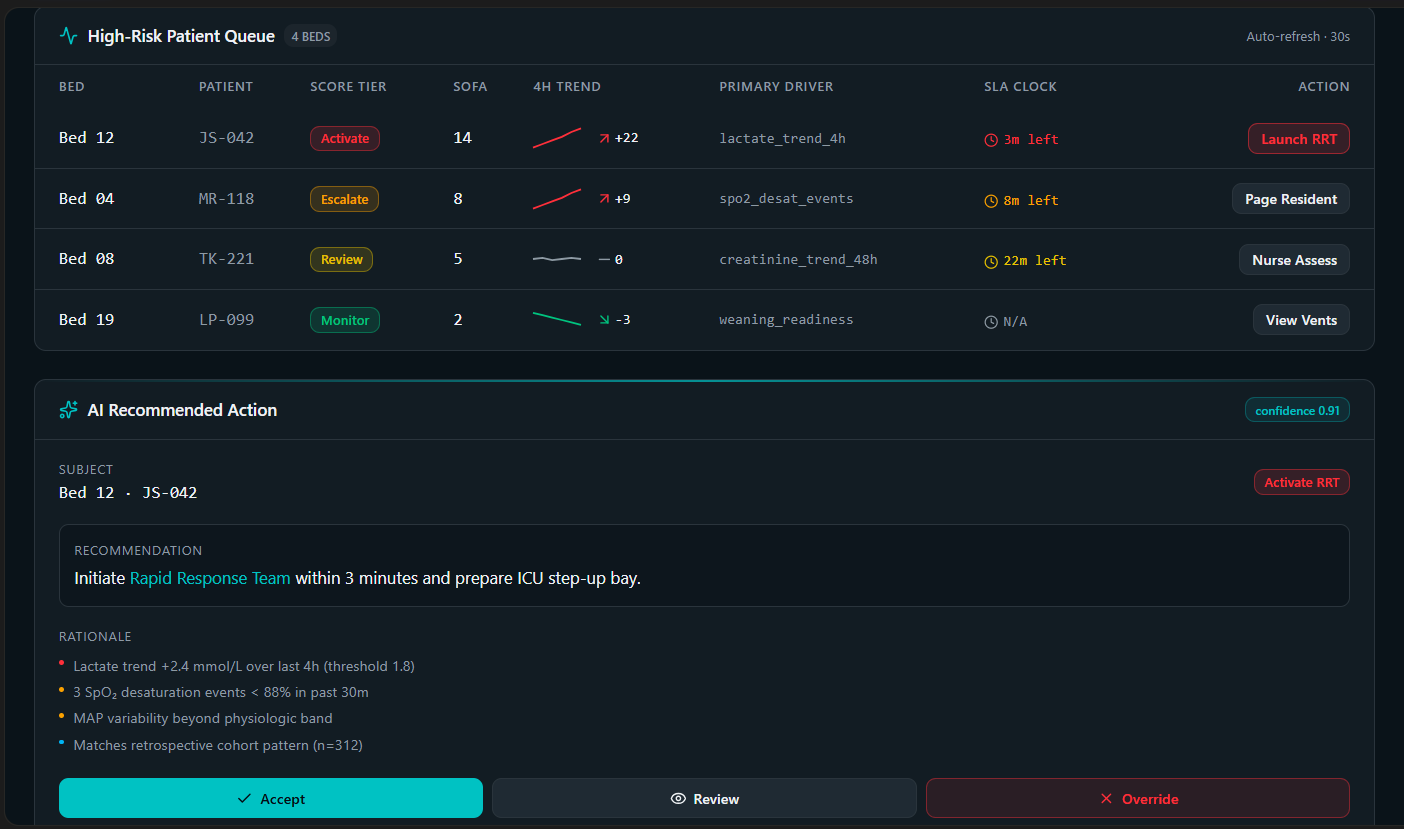
Risk tiering logic
Action-driven tiers: Monitor, Review, Escalate, Activate.
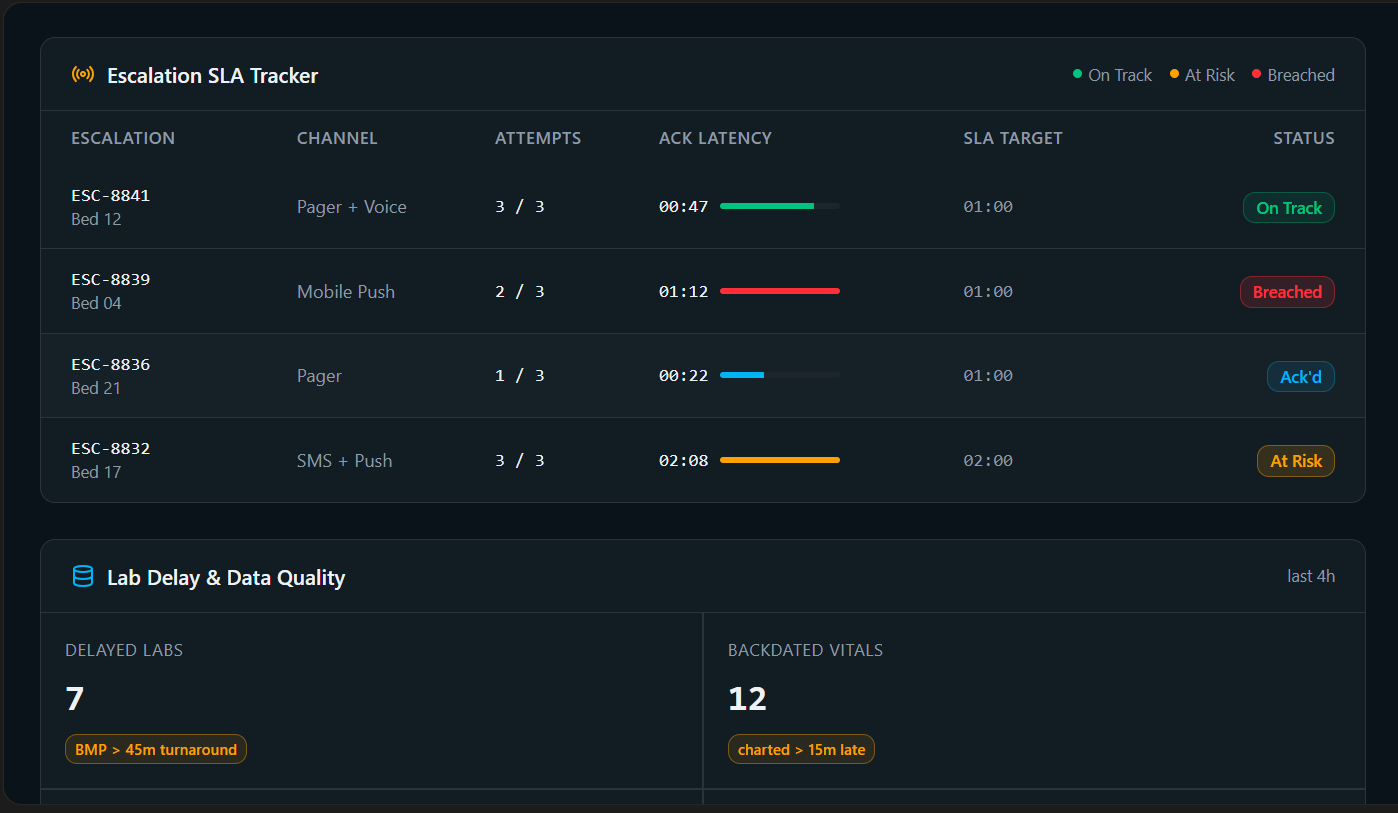
SLA escalation model
Routes signals with timers and auto-escalation on breach.
Dashboard prototype
Role-based views for nurses, residents, and ops.
Human override loop
Clinicians can downgrade, defer, or document decisions.
From raw signals to auditable workflow
A vertical pipeline. Each layer adds structure, accountability, or visibility — and feeds the next.
Data Sources
Vitals · Labs · EMR Notes · Alarms · Handoffs · Ventilator Data
Signal Audit Trail
Generated → Detected → Acknowledged → Action Initiated → Action Completed
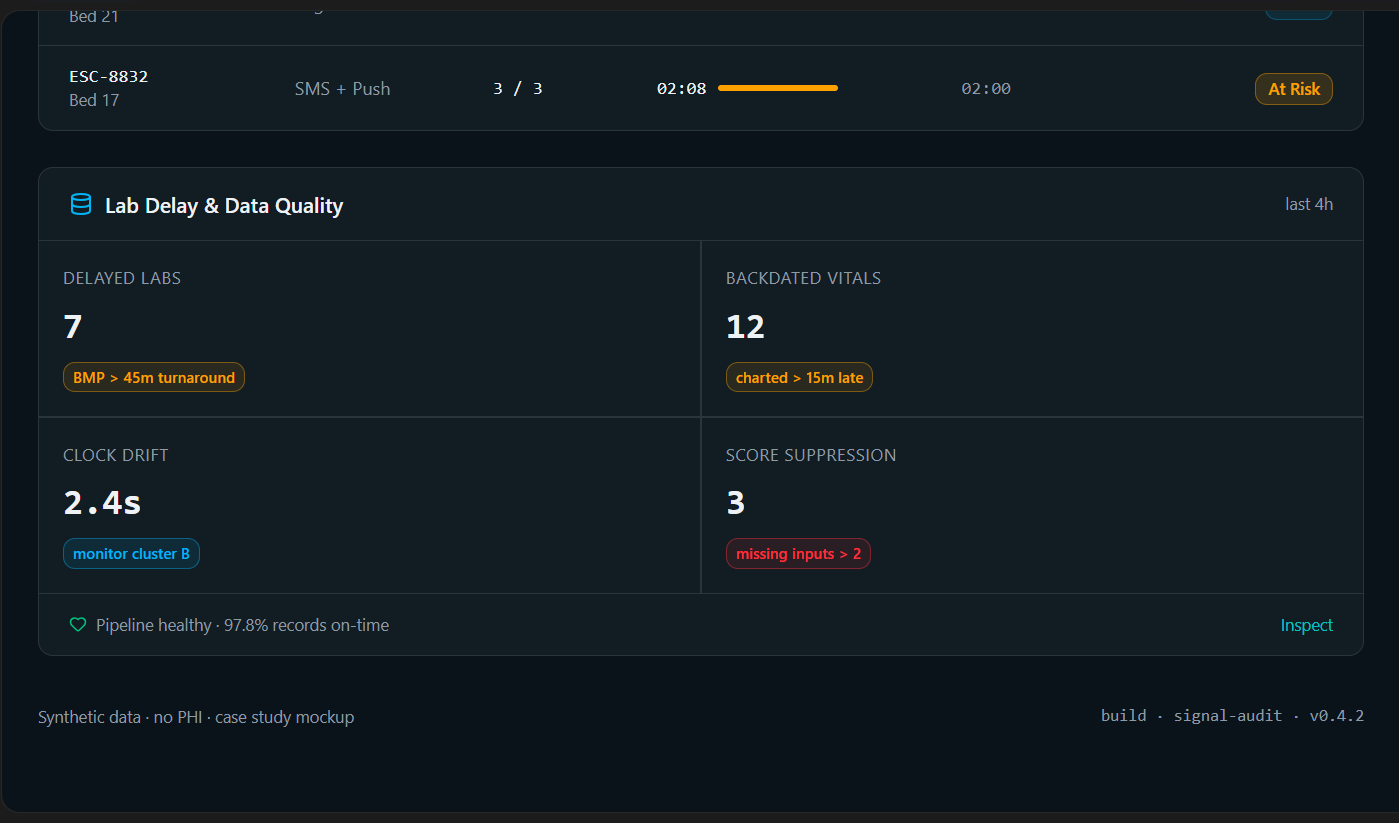
Data Quality Layer
Missing values · backdated vitals · clock drift · impossible values · incomplete notes
Workflow Risk Layer
Monitor · Review · Escalate · Activate
Escalation State Machine
Pending → Acknowledged → Action Initiated → Completed, with SLA breach auto-escalation
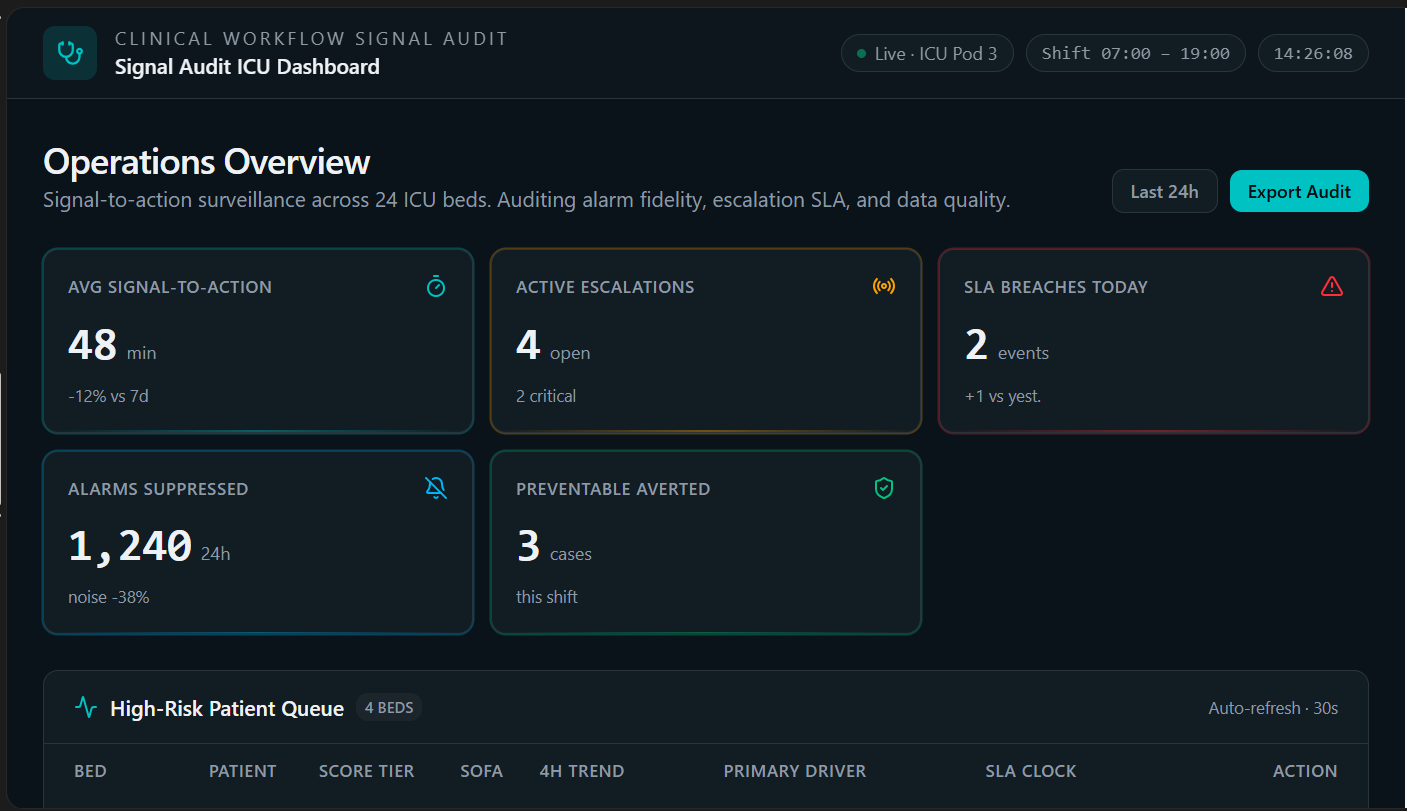
Dashboard Layer
Patient queue · SLA tracker · lab delays · documentation gaps · recommended actions
Audit Feedback Loop
Clinician override · outcome review · bottleneck analysis · quality improvement
Action-driven tiers, not severity scores
Each tier is defined by the response it requires — making escalation decisions easier to route, time, and audit.
| Tier | Meaning | Required action |
|---|---|---|
| Monitor | No immediate workflow risk | Routine observation |
| Review | Signal needs nurse review | Nurse assessment within 30 minutes |
| Escalate | Signal needs clinician action | Resident / order review within 15 minutes |
| Activate | Critical workflow risk | RRT / attending response within 5 minutes |
Role-based views for the people who run the shift
Synthetic data only — no PHI. Screens shown at full fidelity from the working prototype.
From scattered signals to a structured workflow
What this portfolio demo delivers
A synthetic demo, scoped to show end-to-end workflow thinking — not real clinical outcomes.
- Created a synthetic ICU workflow dataset
- Built an audit trail from signal generation to completed action
- Added checks for missing data, impossible values, clock drift, and backdated documentation
- Designed action-driven risk tiers
- Added SLA tracking and routing logic
- Created a dashboard prototype for nurse managers, charge nurses, residents, and operations teams
- Included a human override loop
- Packaged the workflow into a reusable healthtech product concept
A cross-functional approach to healthcare AI
Clinical workflow thinking
Mapping real shift mechanics — handoffs, rounds, escalation paths.
Data systems thinking
Modeling signals, actions, and SLAs as first-class entities.
AI product thinking
Positioning AI as workflow intelligence, not a black-box diagnosis.
UX thinking
Role-based views that match what each user actually decides.
Implementation thinking
Pipeline, schema, state machine, and dashboard wired end-to-end.
Synthetic data. Workflow intelligence. No diagnostic claims.
This demo uses synthetic data only. It does not use real patient records, protected health information, or hospital-identifiable data. It is positioned as workflow intelligence, not diagnostic AI. It supports clinical teams by improving visibility into signal flow, escalation timing, and operational gaps.
Interested in workflow-first healthcare AI systems?
I design structured workflows, data logic, and AI-assisted systems that help clinical and healthtech teams turn fragmented operational signals into usable decision pathways.